


 Sign Out
Sign Out




Pharmacology: Pharmacodynamics: Mechanism of action: Spiolto Respimat: Spiolto Respimat is a fixed dose combination inhalation solution containing a long acting muscarinic receptor antagonist, tiotropium and a long acting beta2-adrenergic agonist, olodaterol (LAMA/LABA) which is delivered via the Spiolto Respimat soft mist inhaler device.
The two active ingredients provide additive bronchodilation due to their different mode of action. Since muscarinic receptors appear to be more prominent in the central airways while β2 adrenoceptors have a higher expression level in the peripheral airways, a combination of tiotropium and olodaterol should provide optimal bronchodilatation in all regions of the lungs.
Tiotropium: Tiotropium bromide is a long-acting, specific antagonist at muscarinic receptors. It has similar affinity to the subtypes, M1 to M5. In the airways, tiotropium bromide competitively and reversibly binds to the M3 receptors in the bronchial smooth musculature, antagonising the cholinergic (bronchoconstrictive) effects of acetylcholine, resulting in bronchial smooth muscle relaxation. The effect was dose dependent and lasted longer than 24h. As an N-quaternary anticholinergic, tiotropium bromide is topically (broncho-) selective when administered by inhalation, demonstrating an acceptable therapeutic range before systemic anticholinergic effects may occur.
Olodaterol: Olodaterol has a high affinity and high selectivity to the human beta2-adrenoceptor.
In vitro studies have shown that olodaterol has 241-fold greater agonist activity at beta2-adrenoceptors compared to beta1-adrenoceptors and 2299-fold greater agonist activity compared to beta3-adrenoceptors. The compound exerts its pharmacological effects by binding and activation of beta2-adrenoceptors after topical administration by inhalation.
Activation of these receptors in the airways results in a stimulation of intracellular adenyl cyclase, an enzyme that mediates the synthesis of cyclic-3',5' adenosine monophosphate (cAMP). Elevated levels of cAMP induce bronchodilation by relaxation of airway smooth muscle cells.
Olodaterol has the pre-clinical profile of a long-acting selective beta2-adrenoceptor agonist (LABA) with a fast onset of action and duration of action of at least 24 hours.
Beta-adrenoceptors are divided into three subtypes, beta1-adrenoceptors predominantly expressed on cardiac muscle, beta2-adrenoceptors predominantly expressed on airway smooth muscle and beta3-adrenoceptors predominantly expressed on adipose tissue. Beta2-agonists cause bronchodilation. Although the beta2-adrenoceptor is the predominant adrenergic receptor in the airway smooth muscle it is also present on the surface of a variety of other cells, including lung epithelial and endothelial cells and in the heart. The precise function of beta2-receptors in the heart is not known, but their presence raises the possibility that even highly selective beta2-adrenergic agonists may have cardiac effects.
Effects on cardiac electrophysiology: Tiotropium: In a dedicated QT study involving 53 healthy volunteers, tiotropium inhalation powder 18 microgram and 54 microgram (i.e. three times the therapeutic dose) over 12 days did not significantly prolong QT intervals of the ECG.
Olodaterol: The effect of olodaterol on the QT/QTc interval of the ECG was investigated in 24 healthy male and female volunteers in a double-blind, randomised, placebo- and active (moxifloxacin) controlled study. Olodaterol at single doses of 10, 20, 30 and 50 microgram, demonstrated that compared with placebo, the mean changes from baseline in QT interval over 20 minutes to 2 hours after dosing increased dose-dependently from 1.6 (10 microgram olodaterol) to 6.5 ms (50 microgram olodaterol), with the upper limit of the two-sided 90% confidence intervals being less than 10 ms at all dose levels for individually corrected QT (QTcI).
The effect of 5 microgram and 10 microgram olodaterol on heart rate and rhythm was assessed using continuous 24-hour ECG recording (Holter monitoring) in a subset of 772 patients in the 48-week, placebo-controlled Phase 3 Trials. There were no dose- or time-related trends or patterns observed for the magnitudes of mean changes in heart rate or premature beats. Shifts from baseline to the end of treatment in premature beats did not indicate meaningful differences between olodaterol 5 microgram, 10 microgram and placebo.
Spiolto Respimat: Two 52-week randomized, double-blind trials using SPIOLTO RESPIMAT enrolled 5162 patients with COPD. In a pooled analysis the number of subjects with changes from baseline-corrected QTcF (Fridericia correction) interval of >30 msec at 40 minutes post-dose on day 85, 169, and 365, ranged from 3.1%, 4.7%, and 3.6% for the SPIOLTO RESPIMAT group compared to 4.1%, 4.4%, and 3.6% for olodaterol 5 microgram and 3.4%, 2.3%, and 4.6% for the tiotropium 5 microgram group, respectively.
Clinical efficacy and safety: The Phase III clinical development program for SPIOLTO RESPIMAT included three randomised, double-blind trials: (i) two replicate, 52 week parallel group trials comparing SPIOLTO RESPIMAT with tiotropium 5 microgram and olodaterol 5 microgram (1029 received SPIOLTO RESPIMAT) [Trials 1 and 2]; (ii) one 6 week cross-over trial comparing SPIOLTO RESPIMAT with tiotropium 5 microgram and olodaterol 5 microgram and placebo (139 received SPIOLTO RESPIMAT) [Trial 3].
In these trials, the comparator products, tiotropium 5 microgram, olodaterol 5 microgram and placebo, were administered via the Respimat inhaler.
Patient characteristics: The majority of the 5162 patients recruited in the global, 52 week trials [Trials 1 and 2] were male (73%), white (71%) or Asian (25%), with a mean age of 64.0 years. Mean post-bronchodilator FEV1 was 1.37 L (GOLD 2 [50%], GOLD 3 [39%], and GOLD 4 [11%]). Mean β2-agonist responsiveness was 16.6% of baseline (0.171 L). Pulmonary medications allowed as concomitant therapy included inhaled steroids [47%] and xanthines [10%].
The 6 week trial [Trial 3] was conducted in Europe and North America. The majority of the 219 recruited patients were male (59%) and white (99%), with a mean age of 61.1 years. Mean post-bronchodilator FEV1 was 1.55 L (GOLD 2 [64%], GOLD 3 [34%], GOLD 4 [2%]). Mean β2-agonist responsiveness was 15.9% of baseline (0.193 L). Pulmonary medications allowed as concomitant therapy included inhaled steroids [41%] and xanthines [4%].
Effects on Lung function: In the 52 week trials, SPIOLTO RESPIMAT administered once daily in the morning, provided clear improvement in lung function within 5 minutes after the first dose compared to tiotropium 5 microgram (mean increase in FEV1 of 0.137 L for SPIOLTO RESPIMAT vs. 0.058 L for tiotropium 5 microgram [p<0.0001] and 0.125 L for olodaterol 5 microgram [p=0.16]).
In both studies, significant improvements were observed in FEV1 AUC0-3h response and trough FEV1 response after 24 weeks (lung function primary endpoints) for SPIOLTO RESPIMAT compared to tiotropium 5 microgram and olodaterol 5 microgram (see Table 1).
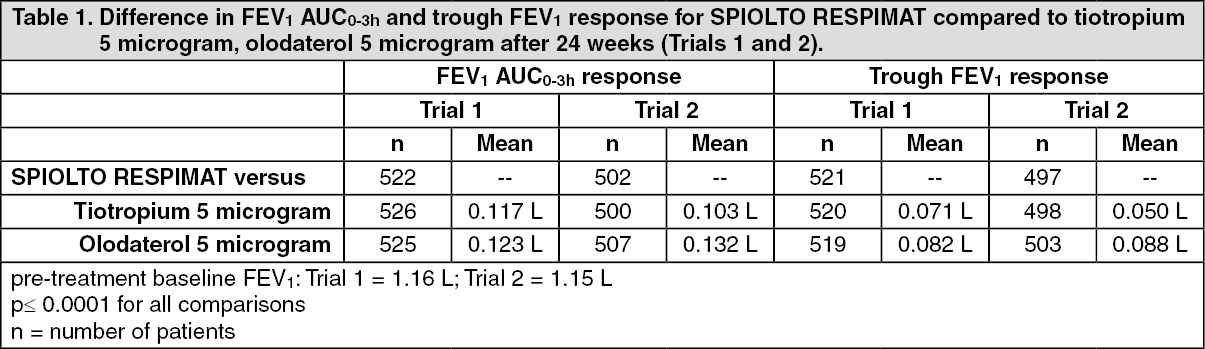 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients with a higher degree of reversibility at baseline generally exhibited a higher bronchodilator response with SPIOLTO RESPIMAT than patients with a lower degree of reversibility at baseline.
The increased bronchodilator effects of SPIOLTO RESPIMAT compared to tiotropium 5 microgram and olodaterol 5 microgram were maintained throughout the 52 week treatment period. SPIOLTO RESPIMAT also improved morning and evening PEFR (peak expiratory flow rate) compared to tiotropium 5 microgram and olodaterol 5 microgram as measured by patient's daily recordings.
In the 6 week trial, SPIOLTO RESPIMAT showed a significantly greater FEV1 response compared to tiotropium 5 microgram, olodaterol 5 microgram and placebo (p<0.0001) over the full 24 hour dosing interval (see Table 2).
 Click on icon to see table/diagram/image
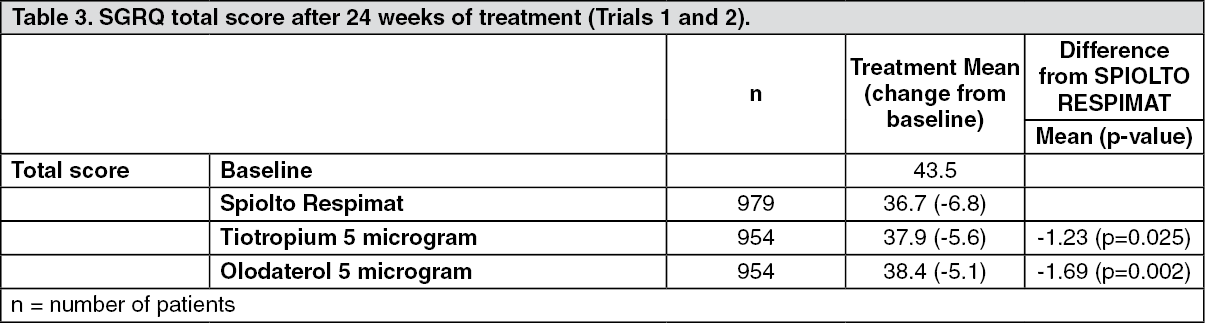
Click on icon to see table/diagram/imageHealth-related Quality of Life: SPIOLTO RESPIMAT showed improvement in health-related quality of life as indicated by a reduction in St. George Respiratory Questionnaire (SGRQ) total score. After 24 weeks (Trials 1 and 2), there was a statistically significant improvement in mean SGRQ total score for SPIOLTO RESPIMAT compared to tiotropium 5 microgram and olodaterol 5 microgram (Table 3); improvements were seen in all SGRQ domains. More patients treated with SPIOLTO RESPIMAT had a clinically meaningful improvement in SGRQ total score (MCID, defined as a decrease of at least 4 units from baseline) compared to tiotropium 5 microgram (57.5% vs. 48.7%, p=0.0001) and olodaterol 5 microgram (57.5% vs. 44.8%, p<0.0001). (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn two additional 12-week (Trials 7 and 8), placebo-controlled clinical trials, SGRQ total score at 12 weeks was also included as primary endpoint as a measure of health-related quality of life.
In the 12-week trials, SPIOLTO RESPIMAT demonstrated an improvement compared with placebo at week 12 in mean SGRQ total score (primary endpoint) of -4.9 (95% CI: -6.9, -2.9; p<0.0001) and -4.6 (95% CI: -6.5, -2.6; p<0.0001). In a pooled analysis of the 12-week trials, the proportion of patients with a clinically meaningful decrease in SGRQ total score (defined as a decrease of at least 4 units from baseline) at week 12 was greater for SPIOLTO RESPIMAT (52%) compared with tiotropium 5 microgram (41%; odds ratio: 1.56 (95% CI: 1.17, 2.07), p=0.0022) and placebo (32%; odds ratio: 2.35 (95% CI: 1.75, 3.16), p <0.0001).
In Trial 9, treatment with SPIOLTO RESPIMAT provided improvements in the COPD Assessment Test score (CAT, a measure of health-related quality of life) versus tiotropium 5 microgram at all study visits (adjusted mean difference versus tiotropium from -0.7 (95% CI (-1.0, -0.5)) at day 90 to -0.4 (95% CI (-0.7, -0.1)) at day 360, all p<0.01). In a responder analysis the proportion of patients experiencing a clinically meaningful improvement in CAT (defined as a reduction of 2 points or more) was larger with SPIOLTO RESPIMAT versus tiotropium 5 microgram (44.51% vs 40.77% respectively, odds ratio 1.17, 95% CI 1.06-1.28 p<0.001).
Dyspnoea: After 24 weeks (Trials 1 and 2), mean TDI focal score was 1.98 units for SPIOLTO RESPIMAT, with a significant improvement compared to tiotropium 5 microgram (mean difference 0.36, p=0.008) and olodaterol 5 microgram (mean difference 0.42 (p=0.002).
More patients treated with SPIOLTO RESPIMAT had a clinically meaningful improvement in TDI focal score (MCID, defined as a value of at least 1 unit) compared to tiotropium 5 microgram (54.9% vs. 50.6%, p=0.0546) and olodaterol 5 microgram (54.9% vs. 48.2%, p=0.0026).
Rescue Medication Use: Patients treated with SPIOLTO RESPIMAT used less daytime and night-time rescue salbutamol compared to patients treated with tiotropium 5 microgram and olodaterol 5 microgram (mean daytime rescue use for SPIOLTO RESPIMAT of 0.76 occasions per day compared to 0.97 occasions per day for tiotropium 5 microgram and 0.87 occasions per day for olodaterol 5 microgram, p<0.0001; mean nighttime rescue use for SPIOLTO RESPIMAT of 1.24 occasions per day compared to 1.69 occasions per day for tiotropium 5 microgram and 1.52 occasions per day for olodaterol 5 microgram, p<0.0001) [(Trials 1 and 2)].
Patient Global Rating: Patients treated with SPIOLTO RESPIMAT perceived a greater improvement in their respiratory condition compared to tiotropium 5 microgram and olodaterol 5 microgram, as measured by a Patient's Global Rating (PGR) scale (Trials 1 and 2).
Exacerbations: Tiotropium 5 microgram has previously demonstrated a statistically significant reduction in risk of a COPD exacerbation compared to placebo. COPD exacerbations was included as an additional endpoint in the 52 week pivotal trials (Trials 1 and 2). In the combined dataset, the proportion of patients experiencing a moderate/severe COPD exacerbation was 27.7% for SPIOLTO RESPIMAT and 28.8% for tiotropium 5 microgram (p=0.39). These studies were not specifically designed to evaluate the effect of treatments on COPD exacerbations.
In a one-year, randomised, double-blind, active-controlled parallel group clinical trial (Trial 9) SPIOLTO RESPIMAT was compared with tiotropium 5 microgram on COPD exacerbations. All respiratory medications except anticholinergics, long-acting beta-agonists and combinations thereof were allowed as concomitant treatment, i.e. rapidly acting beta-agonists, inhaled corticosteroids and xanthines. The primary endpoint was the annualised rate of moderate to severe COPD exacerbations (3939 patients received SPIOLTO RESPIMAT and 3941 patients received tiotropium 5 microgram).
The majority of patients were male (71.4%) and Caucasian (79.3%). The mean age was 66.4 years, mean post-bronchodilator FEV1 was 1.187 L (SD 0.381), and 29.4% of patients had a history of clinically important cardiovascular disease.
Exacerbations of COPD were defined as "a complex of lower respiratory events/symptoms (increase or new onset) related to the underlying COPD, with duration of three days or more, requiring a prescription of antibiotics and/or systemic steroids and/or hospitalisation".
SPIOLTO RESPIMAT treatment resulted in an additional 7% reduction in the annualised rate of moderate to severe COPD exacerbation in comparison to tiotropium 5 microgram (rate ratio (RR) 0.93, 99% Confidence Interval (CI), 0.85-1.02, p=0.0498). The study was designed to reach a significance level of 1%.
SPIOLTO RESPIMAT treatment resulted reduction in an 11% lower annualised rate of hospitalisations due to a COPD exacerbation (RR 0.89, 95% CI 0.76-1.03, p=0.1265). Beyond this SPIOLTO RESPIMAT treatment resulted in a 20% lower annualised rate of moderate to severe exacerbation that required treatment with systemic corticosteroids (RR 0.80, 95% CI 0.68-0.94, p=0.0068) and in a 9% lower annualised rate of moderate to severe exacerbation that required treatment with systemic corticosteroids and antibiotics (RR 0.91, 95% Cl 0.83-1.00, p=0.0447). Treatment with SPIOLTO RESPIMAT did not result in a reduction in the rate of moderate to severe exacerbations treated with antibiotics only (RR 1.07, 95% CI 0.96-1.20, p=0.2062).
Time to all-cause mortality was included as a secondary endpoint in this trial. There was no significant difference in the risk of all-cause mortality between SPIOLTO RESPIMAT and tiotropium 5 microgram. During the actual treatment period (i.e. on-treatment plus one day) 36 versus 32 deaths were observed (Hazard Ratio (HR) 1.09, 95% CI, 0.67, 1.75, p=0.7357) while during the planned study period (381 days) 107 versus 121 deaths were observed (HR 0.88, 95% CI, 0.68, 1.15, p=0.3485) for SPIOLTO RESPIMAT and tiotropium 5 microgram, respectively.
The analysis of the additional exacerbation trial (Trial 9) is displayed in Table 4. (See Table 4.)
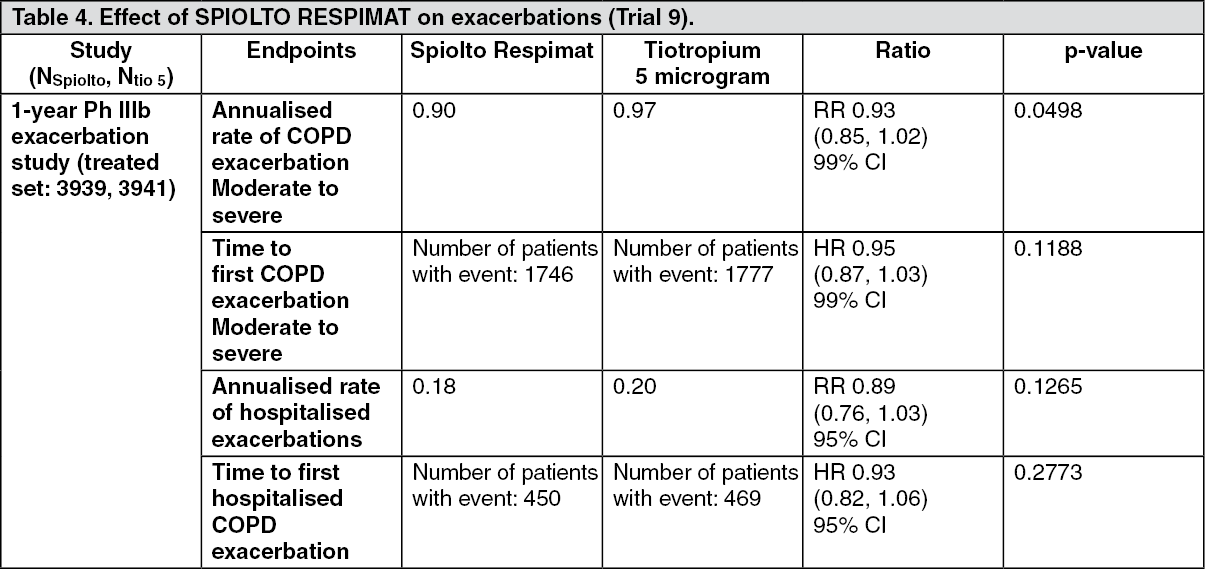 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageInspiratory capacity, breathing discomfort and exercise endurance: The effect of SPIOLTO RESPIMAT on inspiratory capacity, breathing discomfort and symptom-limited exercise endurance was investigated in three randomised, double-blind trials in COPD patients: (i) two replicate, 6 week cross-over trials comparing SPIOLTO RESPIMAT with tiotropium 5 microgram, olodaterol 5 microgram and placebo during constant work rate cycling (450 received SPIOLTO RESPIMAT) [Trials 4 and 5]; (ii) one 12 week parallel group trial comparing SPIOLTO RESPIMAT with placebo during constant work rate cycling (139 received SPIOLTO RESPIMAT) and constant speed walking (sub-set of patients) [Trial 6].
SPIOLTO RESPIMAT significantly improved inspiratory capacity at rest two hours post-dose compared to tiotropium 5 microgram (0.114 L, p<0.0001; Trial 4, 0.088 L, p=0.0005; Trial 5), olodaterol 5 microgram (0.119 L, p<0.0001; Trial 4, 0.080 L, p=0.0015; Trial 5) and placebo (0.244 L, p<0.0001; Trial 4, 0.265 L, p<0.0001; Trial 5) after 6 weeks.
In Trials 4 and 5, SPIOLTO RESPIMAT significantly improved endurance time during constant work rate cycling compared to placebo after 6 weeks (Trial 4: geometric mean endurance time of 454 s for SPIOLTO RESPIMAT compared to 375 seconds for placebo (20.9% improvement, p<0.0001); Trial 5: geometric mean endurance time of 466 seconds for SPIOLTO RESPIMAT compared to 411 seconds for placebo (13.4% improvement, p<0.0001).
In Trial 6, SPIOLTO RESPIMAT significantly improved endurance time during constant work rate cycling compared to placebo after 12 weeks (geometric endurance time of 528 seconds for SPIOLTO RESPIMAT compared to 464 seconds for placebo (13.8% improvement, p=0.021).
Pharmacokinetics: General Introduction: When tiotropium and olodaterol were administered in combination by the inhaled route, the pharmacokinetic parameters for each component were similar to those observed when each active substance was administered separately.
Tiotropium and olodaterol demonstrate linear pharmacokinetics in the therapeutic range. On repeated once-daily inhalation administration, steady state of tiotropium is reached by day 7. Steady state of olodaterol is achieved after 8 days of once-daily inhalation, and accumulation is up to 1.8-fold as compared to a single dose.
General Characteristics of the Active Substance after Administration of the Medicinal Product: Absorption: Tiotropium: Urinary excretion data from young healthy volunteers suggests that approximately 33% of the dose inhaled via the RESPIMAT inhaler reaches the systemic circulation. The absolute bioavailability from an orally administered solution was found to be 2-3%. Maximum tiotropium plasma concentrations are observed 5-7 minutes after the inhalation via RESPIMAT.
Olodaterol: In healthy volunteers the absolute bioavailability of olodaterol following inhalation was estimated to be approximately 30%, whereas the absolute bioavailability was below 1% when given as an oral solution. Maximum olodaterol plasma concentrations generally are reached within 10 to 20 minutes following drug inhalation via RESPIMAT.
Distribution: Tiotropium has a plasma protein binding of 72% and shows a volume of distribution of 32 L/kg. Studies in rats have shown that tiotropium does not penetrate the blood-brain barrier to any relevant extent.
Olodaterol has a plasma protein binding of approximately 60% and shows a volume of distribution of 1110 L. Olodaterol is a substrate for the P-gp, OAT1, OAT3 and OCT1 transporter. Olodaterol is not a substrate for the following transporters: BCRP, MRP, OATP2, OATP8, OATP-B, OCT2 and OCT3.
Biotransformation: Tiotropium: The extent of metabolism is small. This is evident from 74% of an intravenous dose being excreted in the urine as unchanged drug. The ester tiotropium is nonenzymatically cleaved into its alcohol and acid component (N-methylscopine and dithienylglycolic acid, respectively), both not binding to muscarinic receptors. In vitro experiments with human liver microsomes and human hepatocytes suggest that some further drug (<20% of the dose after intravenous administration) is metabolized by cytochrome P450 (CYP) 2D6 and 3A4 dependent oxidation and subsequent glutathione conjugation to a variety of Phase II-metabolites.
Olodaterol is substantially metabolized by direct glucuronidation and by O-demethylation at the methoxy moiety followed by conjugation. Of the six metabolites identified, only the unconjugated demethylation product (SOM 1522) binds to β2-receptors; this metabolite however is not detectable in plasma after chronic inhalation of the recommended therapeutic dose or doses of up to 4-fold higher. Cytochrome P450 isozymes CYP2C9 and CYP2C8, with negligible contribution of CYP3A4, are involved in the O-demethylation of olodaterol, while uridine diphosphate glycosyl transferase isoforms UGT2B7, UGT1A1, 1A7 and 1A9 were shown to be involved in the formation of olodaterol glucuronides.
Elimination: Tiotropium: Intravenously administered tiotropium is mainly excreted unchanged in urine (74%). The total clearance in healthy volunteers is 880 mL/min. After inhalation by COPD patients to steady-state, urinary excretion is 18.6% of the dose, the remainder being mainly non-absorbed drug in gut that is eliminated via the faeces. The renal clearance of tiotropium exceeds the glomerular filtration rate, indicating active secretion into the urine. The effective half-life of tiotropium following inhalation by COPD patients ranges between 27 and 45 h.
Olodaterol: Total clearance of olodaterol in healthy volunteers is 872 mL/min, and renal clearance is 173 mL/min. Following intravenous administration of [14C]-labelled olodaterol, 38% of the radioactive dose was recovered in the urine and 53% was recovered in feces. The amount of unchanged olodaterol recovered in the urine after intravenous administration was 19%. Following oral administration, only 9% of the radioactivity (0.7% unchanged olodaterol) was recovered in urine, while the major portion was recovered in feces (84%). More than 90% of the dose was excreted within 6 and 5 days following intravenous and oral administration, respectively. Following inhalation, excretion of unchanged olodaterol in urine within the dosing interval in healthy volunteers at steady state accounted for 5-7% of the dose. Olodaterol plasma concentrations after inhalation decline in a multiphasic manner with a terminal half-life of approximately 45 hours.
Characteristics in Patients: Tiotropium: As expected for all predominantly renally excreted drugs, advancing age was associated with a decrease of tiotropium renal clearance from 347 mL/min in COPD patients <65 years to 275 mL/min in COPD patients ≥65 years. This did not result in a corresponding increase in AUC0-6,ss or Cmax,ss values.
Olodaterol: A pharmacokinetic meta-analysis utilizing data from 2 controlled clinical trials that included 405 patients with COPD and 296 patients with asthma showed that no dose adjustment is necessary due to effects of age, gender and weight on systemic exposure to olodaterol.
Race: Olodaterol: Comparison of pharmacokinetic data within and across studies with olodaterol revealed a trend for higher systemic exposure in Japanese and other Asians than in Caucasians.
No safety concerns were identified in clinical studies with olodaterol in Caucasians and Asians of up to one year with olodaterol Respimat at doses up to twice the recommended therapeutic dose.
Renal Insufficiency: Tiotropium: Following once daily inhaled administration of tiotropium to steady-state in COPD patients with mild renal impairment (CrCl 50-80 mL/min) resulted in slightly higher AUC0-6,ss (between 1.8 to 30% higher) and similar Cmax,ss compared to patients with normal renal function (CrCl >80 mL/min). In subjects with moderate to severe renal impairment (CrCl <50 mL/min) intravenous administration of tiotropium resulted in twofold higher total exposure (82% higher AUC0-4h and 52% higher Cmax) compared to subjects with normal renal function, which was confirmed by observations after dry powder inhalation.
Olodaterol: There were no clinically relevant increases of systemic exposure in patients with renal impairment.
Hepatic Insufficiency: Tiotropium: Liver insufficiency is not expected to have any relevant influence on tiotropium pharmacokinetics. Tiotropium is predominantly cleared by renal elimination (74% in young healthy volunteers) and simple non-enzymatic ester cleavage to pharmacologically inactive products.
Olodaterol: There was no evidence for differences in elimination of olodaterol, nor did protein binding differ, between subjects with mild or moderate hepatic impairment and their healthy controls. A study in subjects with severe hepatic impairment was not performed.
Toxicology: Preclinical safety data: Tiotropium + olodaterol: Effects in non-clinical studies with the combination tiotropium/olodaterol were observed only at exposures considered sufficiently in excess of the maximum human exposure indicating little relevance to clinical use.
Tiotropium: Studies on genotoxicity and carcinogenic potential revealed no special hazard for humans. Harmful effects with respect to pregnancy, embryonal/foetal development, parturition or postnatal development could only be demonstrated at maternally toxic dose levels. Tiotropium bromide was not teratogenic in rats or rabbits. The respiratory (irritation) and urogenital (prostatitis) changes and reproductive toxicity were observed at local or systemic exposures more than five-fold the therapeutic exposure.
Olodaterol: Studies on genotoxicity and carcinogenic potential revealed no special hazard for humans. Increased incidences were observed of mesovarian leiomyoma in rats and of uterus leiomyoma and leiomyosarcoma in mice. This is considered a class effect which is observed in rodents after long-term exposure to high doses of β2-agonists. Up to now, β2-agonists have not been associated with cancer in humans.
In rats, no teratogenic effects occurred after inhalation at doses of 1054 microgram/kg/day (>2600 times the human exposure (AUC(0-24h)) at the dose of 5 mcg). In pregnant NZW rabbits, an inhalation dose of 2489 microgram/kg/day (approximately 7130 times the human exposure at 5 microgram based on AUC(0-24h)) of olodaterol exhibited fetal toxicity characteristically resulting from beta-adrenoceptor stimulation; these included patchy ossifications, short/bent bones, partially open eye, cleft palate, cardiovascular abnormalities. No significant effects occurred at an inhalation dose of 974 microgram/kg/day (approximately 1353 times the 5 microgram dose based on AUC(0-24h)).